総説1 Intrinsic subtype 分類,分子生物学的リスク分類と病理診断
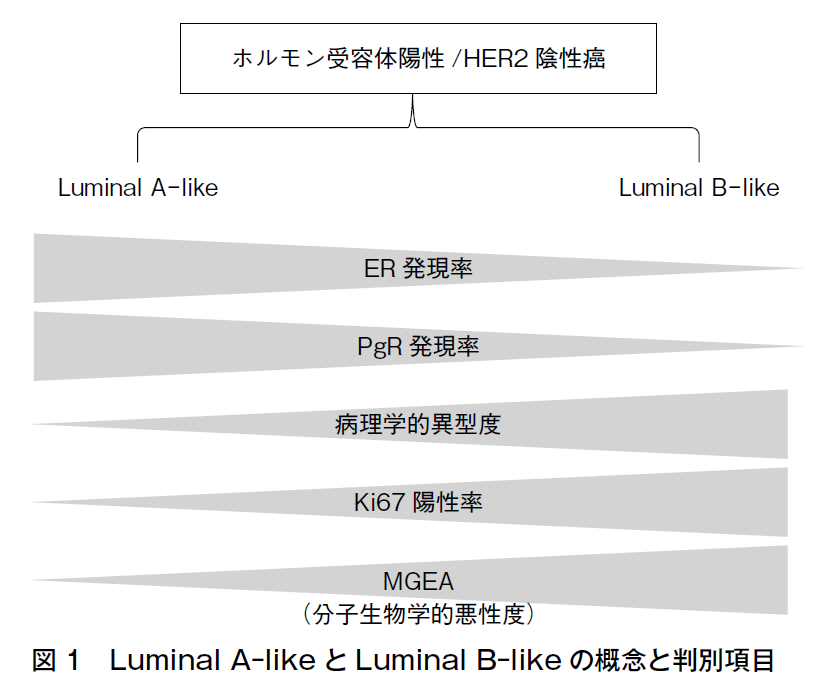
乳癌診療では,腫瘍の浸潤径,腋窩リンパ節転移状況,組織型,病理学的悪性度,エストロゲン受容体(ER)/プロゲステロン受容体(PgR)/HER2状況等の臨床病理学的情報が重要だが,2000年にPerouらがcDNAマイクロアレイを用い乳癌の遺伝子発現プロファイリング(GEP)を行って以来,GEPに基づくintrinsic subtype分類が注目されるようになった1)2)。この分類では,乳癌はLuminal A,Luminal B,HER2-enriched,Basal-like,Normal breast-like等,生物学的性状の異なるサブタイプに分けられる。サブタイプにより予後や薬物感受性が異なるため,薬物療法選択の指標となり得る点が有用だが,GEPを乳癌全例に行うのは臨床上現実的ではない。そこで2011年,2013年,2015年のザンクトガレンコンセンサス会議では,病理学的ER/PgR/HER2/Ki67状況に基づくintrinsic subtypeの代替定義が提唱された3)4)5)。2017年同会議では,HER2-enrichedとbasal-likeは遺伝子解析でのみ定義されるべきものとされ6),現在,日常診療では,ホルモン受容体陽性かつHER2陰性の乳癌のうち,生物学的悪性度の低いものに対しLuminal A-like,高いものに対しLuminal B-like,という形での使用が定着している。Luminal A-likeかLuminal B-likeかの判別に用いられる病理学的項目には,病理学的異型度,ER発現率,PgR発現率,Ki67発現率等がある(図1)。さらに近年,特に欧米で,multi-gene expression assay(MGEA☞乳癌診療ガイドライン①治療編2022年版,薬物CQ11参照)によるリスク分類が重視され,MGEAもLuminal A-like/Luminal B-like判別項目とされている(図1)6)。我が国では,MGEAの一つであるOncotype DXが2023年9月に保険収載となり,今後,普及が加速度的に進むと考えられる。Luminal A-like/Luminal B-like判別に,どの項目を用い,閾値をどこに置くかなど,定義は明確ではなく7),あくまでも便宜的・概念的かつ流動的なものである。そのため,それらの言葉の意味するところについての理解は,診療者間で共有しておかねばならないのはもちろんのことだが,過去の文献を参照する際にも留意する必要がある。
かつてはbasal-likeの代替定義として,ER/PgR/HER2いずれも陰性のいわゆる“triple-negative”が当てられていた3)4)5)。トリプルネガティブ乳癌はGEP上,Basal-like,Luminal-AR(アンドロゲン受容体),immue-activated,claudin-low等,生物学的性質の異なる群に細分化されるが,これらをEGFR,CK5/6,アンドロゲン受容体,細胞接着分子等の発現状況,および腫瘍浸潤リンパ球(TIL)等の病理学的情報に基づき代替的に分類し,治療に役立てようとする試みもなされている。TILのPD-L1発現検索と,その結果に基づく免疫チェックポイント阻害薬の適用が,2019年,保険で認められている(☞病理FRQ5参照)。
乳癌の研究,診断,治療は日進月歩であり,分子生物学的情報と病理学的情報の関係性については今後の動向を注視していく必要がある。
参考文献
1)Perou CM, Sørlie T, Eisen MB, van de Rijn M, Jeffrey SS, Rees CA, et al. Molecular portraits of human breast tumours. Nature. 2000;406(6797):747-52. [PMID:10963602]
2)Sørlie T, Perou CM, Tibshirani R, Aas T, Geisler S, Johnsen H, et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci USA. 2001;98(19):10869-74. [PMID:11553815]
3)Goldhirsch A, Wood WC, Coates AS, Gelber RD, Thürlimann B, Senn HJ;Panel members. Strategies for subtypes--dealing with the diversity of breast cancer:highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann Oncol. 2011;22(8):1736-47. [PMID:21709140]
4)Goldhirsch A, Winer EP, Coates AS, Gelber RD, Piccart-Gebhart M, Thürlimann B, et al;Panel members. Personalizing the treatment of women with early breast cancer:highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann Oncol. 2013;24(9):2206-23. [PMID:23917950]
5)Coates AS, Winer EP, Goldhirsch A, Gelber RD, Gnant M, Piccart-Gebhart M, et al. Tailoring therapies--improving the management of early breast cancer:St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Ann Oncol. 2015;26(8):1533-46. [PMID:25939896]
6)Curigliano G, Burstein HJ, Winer EP, Gnant M, Dubsky P, Loibl S, et al. De-escalating and escalating treatments for early-stage breast cancer:the St. Gallen International Expert Consensus Conference on the Primary Therapy of Early Breast Cancer 2017. Ann Oncol. 2017;28(8):1700-12. [PMID:28838210]
7)Burstein HJ, Curigliano G, Thürlimann B, Weber WP, Poortmans P, Regan MM, et al;Panelists of the St Gallen Consensus Conference. Customizing local and systemic therapies for women with early breast cancer:the St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021. Ann Oncol. 2021;32(10):1216-35. [PMID:34242744]